

A recent report shows that populations with protections—including health insurance, access to health care and other luxuries—do not acquire COVID-19 as much as groups who do not have those protections, including farmworkers, grocery store clerks and nursing home attendants.
According to the Center for the Study of Latino Health and Culture (CESLAC) of the David Geffen School of Medicine at UCLA, social inequalities explain why COVID-19 appears to be so randomly distributed in California.
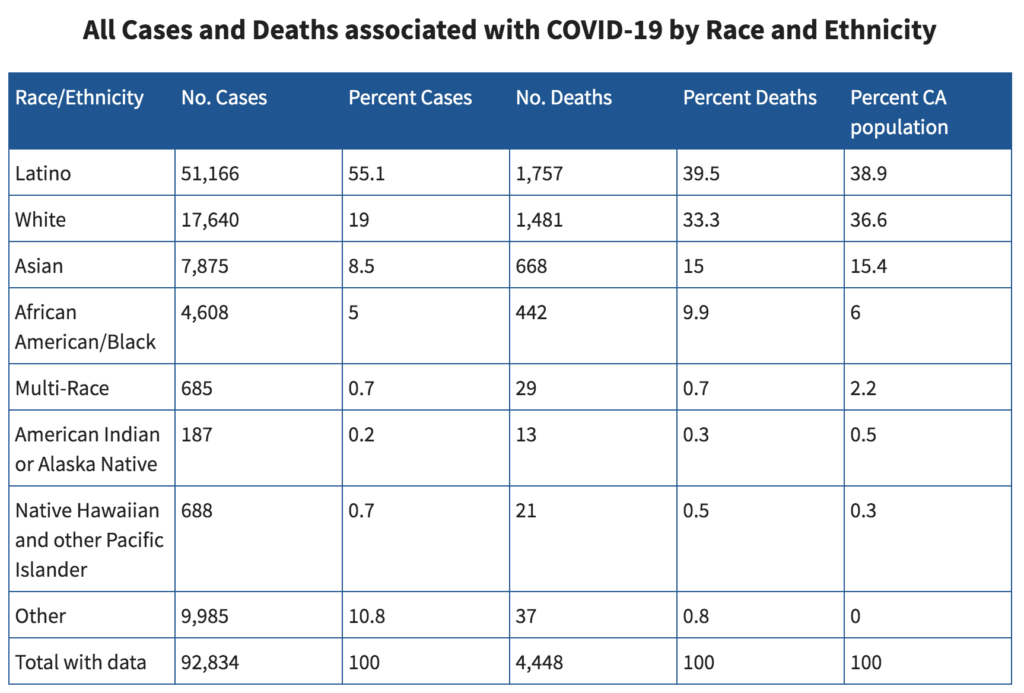
The data indicate that exposure falls most heavily on the state’s Latino, African-American, Asian-American and Pacific Islander populations.
“In an ideal world, there would be no difference in the case rates between the race or ethnic groups,” said Paul Hsu, who teaches epidemiology at UCLA. “But we see major differences in the infection rates of the different groups, indicating that exposure to the coronavirus falls more heavily on some groups than others.”
“Some individuals enjoy a protective social umbrella, with full health insurance, good access to health care, and the ability to shelter at home until the storm passes” said David E. Hayes-Bautista, a distinguished professor of medicine and director of CESLAC. “Others have far fewer protective umbrellas, with big holes in them—such as little or no health insurance, little or no access to medical care—and essential jobs that require them to stay out in the rain so that others can shelter at home.”
In California, these essential jobs are more often than not filled by Latinos and other minorities.
Unsurprisingly, Latinos and Asians have about two times the death rate of non-Hispanic whites in the elderly population—while African Americans have about three times the death rate all within the elderly population.
According to Hayes-Bautista, research found that more middle-aged Latinos, aged 50 to 64, had twice the death rate compared to white individuals in the same age range. While there was not enough data to collect death rates for Black or Asian populations, it can be inferred the pattern holds true.
“What we’re seeing is that the burden is falling disproportionately on populations of color. And in California, with its 40 million population, 62 percent of the population is what we used to call ‘minority’—so if this is not a minority issue, why would there be these differences in death?” said Hayes-Bautista.
It’s a wealth issue.
Hayes-Bautista told Ms. that wealthier populations have the essential goods and services to take necessary procedures against the pandemic.
On the other hand, farmworkers, for example, don’t have these goods. When they grow their own food, they often do so without protective equipment.
Checkout clerks in grocery stores face similar disadvantages: When at work, a checkout person typically has anywhere from 50-200 people pass within 30 inches of the clerk. Yet, if they catch the illness due to the constant spreading of germs and, in turn, are fired because they miss work, they do not have the proper health care to help them through it.
“The general trend is holding up: Those who have access to health care and a physician aren’t doing so bad, but those who have to provide them with those services are the ones paying the price by just being exposed to more people,” explained Hayes-Bautista.
Universal Health Care
Unlike Japan and Germany, the United States does not have a universal health care system. According to Hayes-Bautista, this is playing a role in the spread of COVID to less-wealthy populations: When any person loses their job, their benefits and health care are gone. It is a battle between the private and public sectors.
“There’s a big differential because we rely on private sector health care and the public sector only steps in to fill the gaps, but during a pandemic we do not have the structure to work on a population-based level.”
Like many researchers, Hayes-Bautista and his team are still evaluating the many factors that impact the spread of this disease.
“We’re going down a very steep learning curve and this virus is certainly throwing us some curves. I feel confident that we will learn enough to figure this out, but the question is: How many people will have to die between here and then that didn’t have to die if we knew about this earlier?”


