
If Amy Coney Barrett is confirmed, the next abortion case to reach the Court—maybe a gestational limit, a fetal heartbeat law, a ban on an abortion procedure, or ban on sex and race selection—will likely find a much friendlier audience in this new Supreme Court.
The Supreme Court’s recent decision in June Medical Services, while a narrow win for Louisiana’s abortion clinics, revealed a Supreme Court majority as poised as ever to undermine reproductive rights if given another chance.
Unfortunately, with the loss of feminist icon Justice Ruth Bader Ginsburg and the rushed nomination of Judge Amy Coney Barrett to fill her seat, that second chance is likely to come sooner than many imagined.
Although Barrett and the Republican-led Senate continue to tout the judge’s respect for precedent and adherence to judicial impartiality during her confirmation hearings, her track record tells quite another story.
In 2006, Judge Barrett signed onto an ad in the South Bend Tribune to “oppose abortion on demand and defend the right to life from fertilization to natural death.”
In 2012, she signed onto a statement of protest condemning the Obama Administration’s religious accommodation to the Affordable Care Act’s contraceptive mandate as “morally obtuse.”
And in 2013, she delivered two lectures for anti-abortion student groups and signed onto a second anti-abortion advertisement. It’s worth noting that she omitted much of this history from her initial disclosure to the Senate Judiciary Committee.
While Judge Barrett’s personal views on abortion, contraception and the rights of embryos should be sufficient to raise serious concern, her judicial philosophy and track record do little to reassure. She is a faithful adherent to the late Justice Scalia’s brand of originalism, which would undermine the rights of many who are vulnerable, including women and the LGBTQ community.
Moreover, her writings indicate a readiness to diverge from even established Supreme Court precedent with which she disagrees. In her short time on the Seventh Circuit Court of Appeals, Barrett has already flexed her originalist muscles and signaled anti-choice positions.
Regardless of the deflections and obfuscations at last week’s confirmation hearings, the result of an Amy Coney Barrett confirmation is clear: It will lurch the Court significantly to the right. The tenuous balance struck in June Medical Services will be lost.

The next abortion case to reach the Court—maybe a gestational limit, a fetal heartbeat law, a ban on an abortion procedure, or ban on sex and race selection—will likely find a much friendlier audience in this new Supreme Court.
Under the “best case” scenario, unless the ideological composition of the Court is further altered, Roe will be hollowed out to the point where it will offer little protection against even the most draconian state abortion restrictions.
Moreover, with the addition of Barrett to the Court, reproductive rights advocates should be concerned not only with the loss of abortion rights, but also the future of health insurance, contraception, IVF, stem cell research and even the rights of pregnant women.
What now? The Senate will remain essential in the face of future Supreme Court vacancies (Justices Alito and Thomas are in their 70’s, and Justice Breyer is in his 80’s). But with Roe no longer a meaningful backstop against anti-abortion state laws, progress on reproductive rights will depend increasingly on the legislatures rather than the courts.
At the federal level, the Senate, along with the House and presidency, hold the key to passing the Women’s Health Protection Act, which could codify reproductive rights nation-wide. At the state level, governors and state legislators will become more crucial than ever in shaping access at the local level.
For nearly 50 years, Americans have relied on Roe to do the heavy lifting. No more.
This article originally appeared in the Fall 2020 issue of Ms.
Become a member today to read more reporting like this in print and through our app.
June Medical Services: A Brief Respite for Abortion Rights
The Supreme Court’s decision in June Medical Services holds the line on abortion—for now.
This summer, in June Medical Services v. Russo‘s fractured ruling, the Court struck down Louisiana’s admitting privileges law, which would have shuttered all but one abortion clinic in that state and imperiled access in at least six other states where similar laws were enacted but not in effect.

Chief Justice John Roberts joined the Court’s four liberal justices in finding Louisiana’s law nearly indistinguishable from the one it struck down four years prior in Whole Woman’s Health v. Hellerstedt.
The outcome is worth celebrating: The state’s three clinics will remain open and able to serve the roughly 10,000 Louisiana women who need abortions every year, and similar laws in other states will remain unenforceable. But June Medical represents little more than a brief respite for abortion rights.
Sprinkled throughout the pages of its several dueling opinions are glimpses into the future of abortion rights. That future looks challenging at best.
A History of Supreme Court Precedent on Abortion Rights
The Supreme Court first guaranteed the right to abortion 47 years ago in Roe v. Wade. Writing for a decisive 7-2 majority, Justice Harry Blackmun recognized a nearly unfettered right to abortion during the first trimester of pregnancy, with states permitted to regulate abortions in the second trimester in ways related to the health of the pregnant woman.
Only in the third trimester of pregnancy could states interfere with or outlaw abortion—provided those laws contained exceptions when abortions were necessary to preserve the life or health of the woman.
Nearly 30 years later in Planned Parenthood v. Casey, the Court significantly narrowed the right to abortion. A deeply divided Court determined that states could broadly regulate all previability abortions, provided those regulations didn’t “have the purpose or effect” of placing a “substantial obstacle in the path of a woman seeking an abortion.” This “undue burden test” became the backstop against which abortion restrictions have been tested ever since.
Just four years ago in Whole Woman’s Health, yet another closely divided Court gave teeth to the undue burden test, requiring courts to “consider the burdens a law imposes on abortion access together with the benefits those laws confer” [emphasis mine]. The Court scrutinized the alleged benefits of regulations at issue and clarified that, where a regulation serves no real purpose, it should fail constitutional scrutiny.

Much has happened in the four years since Whole Woman’s Health. The seat left open by Justice Antonin Scalia’s death—held hostage by a Republican Senate in President Barack Obama’s final year in office—was eventually filled by President Donald Trump’s first appointee, Neil Gorsuch.
Trump’s second appointee, Brett Kavanaugh, replaced the vacancy left by the retirement of Justice Anthony Kennedy, who while on the bench was a swing vote in Whole Woman’s Health.
June Medical Leaves Gaping Holes for Future Abortion Battles
June Medical was, in some sense, the perfect test for this new Court. How would this philosophically reconfigured Court react to a nearly identical abortion case?
The answer? By exploiting the wiggle room left by the last Court and shifting to the right. The four liberal justices, led by Justice Stephen Breyer, reaffirmed and faithfully applied the standard elaborated in Whole Woman’s Health.
But Roberts penned his own opinion, agreeing with the outcome that the Louisiana law must fail, but broadcasting his disagreement with Whole Woman’s Health and its bolstering of the undue burden standard. Roberts struck down the Louisiana law, even though he voted to uphold identical restrictions in Whole Women’s Health, because he felt constrained by prece- dent in this nearly duplicate case.
Roberts wrote, “I joined the dissent in Whole Woman’s Health and continue to believe that case was wrongly decided.”
He went on to discredit Whole Woman’s Health, laying the foundation for future anti-abortion litigation. The four dissenting justices, including both Trump appointees, also expressed their hostility toward Whole Woman’s Health, and then went further by refusing to follow it.
Taking its opinions together, June Medical reveals a majority of the justices would abandon the more stringent requirements of Whole Woman’s Health in a future case in favor of a more deferential review of state abortion regulations.
Peppered throughout Roberts’s concurrence and the four dissents are solicitations to anti-abortion lawmakers to provide them another chance to walk back abortion rights.
Justice Samuel Alito’s dissent, joined in relevant part by Gorsuch, Kavanaugh and Clarence Thomas, grudgingly admits the Court is bound by Casey, but flirts with the prospect of “reexamining” that decision, noting that “Louisiana has not asked us to do that.”
Roberts, too, makes mention of the fact that the litigants in June Medical didn’t ask them to revisit Casey. And while extolling the virtues of precedent, Roberts cleverly qualifies his allegiance with a reminder that precedent is not an “inexorable command.”
If confronted with a slightly different set of facts or a different abortion restriction, these five justices—or six, assuming Barrett is confirmed—could severely damage abortion rights.
It’s true that Roberts demonstrated restraint and perhaps a hesitancy to overrule Roe or Casey directly. But he seems open to taking an incremental approach—for example, by refusing to find even the most restrictive regulations unduly burdensome, all while claiming to follow Casey. (Remember: Roberts didn’t think the Texas admitting-privileges law in Whole Woman’s Health was unduly burdensome, even though it would have shuttered three-fourths of the clinics in that state.)
And his record with precedent in the abortion context isn’t perfect either. Roberts voted in a 2007 case to uphold an unnecessary nationwide ban on a fake abortion procedure (so-called partial-birth abortion), though the ban was almost identical to one the Court struck down seven years prior. It also lacked an exception for women’s health, which was clearly required by past precedent.
The fact that June Medical was as closely decided as it was will itself encourage future litigation.
This case should have been a slam dunk, disposed of handily by lower federal courts bound to follow Supreme Court precedent. Instead, the conservative 5th U.S. Circuit Court of Appeals felt free to ignore that precedent and relitigate the facts of the case.
The four dissenting Supreme Court justices were indifferent to this insubordination; and on slightly different facts, Roberts may have turned a blind eye too.
But conservative judges are certainly paying close attention. A panel of the 8th U.S. Circuit Court already made use of Roberts’s concurrence, treating Whole Woman’s Health as bad law and lifting injunctions on a number of extremely restrictive anti-abortion laws in Arkansas.
Rather than closing off avenues of future attack against abortion rights, June Medical threw up a temporary detour while paving the way for more anti-abortion activity.
What Avenues Do Anti-Abortion Advocates Have to Limit Abortion Access?
Even if states pivot away from admitting-privilege laws (which have failed at every turn), or focus less on restrictions aimed at “protecting” women’s health from abortion, they’ve got plenty of options. Abortion foes have cooked up an endless parade of restrictions based on fetal protection, maternal “education” and even disingenuous anti-discrimination principles. These include ever-shorter gestational limits; ever-longer waiting periods; counseling requirements, including warning of bogus health risks like cancer; and prohibiting abortion based on sex, race and fetal anomaly.
And, of course, abortion opponents have sought to make abortion unaffordable, with bans on state and federal funding of abortion, and restrictions on health insurance coverage.
For the past several decades, faced with a Supreme Court that couldn’t quite bring itself to reverse Roe, members of the anti-abortion movement focused their attention on cutting off access. And by every measure, they’ve done a superb job: In the years since Roe, state legislatures have passed well over 1,000 abortion restrictions. In 2019 alone, states introduced more than 375 pieces of anti-abortion legislation. That means some 58 percent of U.S. women of reproductive age now live in states considered hostile to abortion rights.
June Medical provides abortion opponents little reason to slow down their legislative and legal assault. As anti-abortion state legislatures continue to pump out legislation, reproductive rights advocates will be forced to turn to the federal courts for protection.
The Center for Reproductive Rights, the organization that represented the Louisiana clinic, is litigating at least 30 cases, including 16 currently before federal appeals courts. After June Medical, anti-abortion litigators will keep pushing the lower federal courts to flout Supreme Court precedent, and then urge the Supreme Court to take up these cases to resolve the conflicts they have fabricated. The next case may well present five (or six) justices with an opportunity to chip away at Roe and Casey to the point where they are hollow promises.
One or more conservative replacements—such as Barrett—could very well cement a more dramatic downfall for abortion rights, giving the dissenting justices in June Medical a fifth vote without the need to bring Roberts along incrementally.
Reason for Optimism in the Fight for Abortion Rights
If we broaden our gaze, however, there’s reason for optimism. Just as anti-abortion activists have focused on access, so too can the reproductive rights movement. That progress doesn’t depend on the Supreme Court, but rather on state legislators, governors and even state judges interpreting state constitutions.
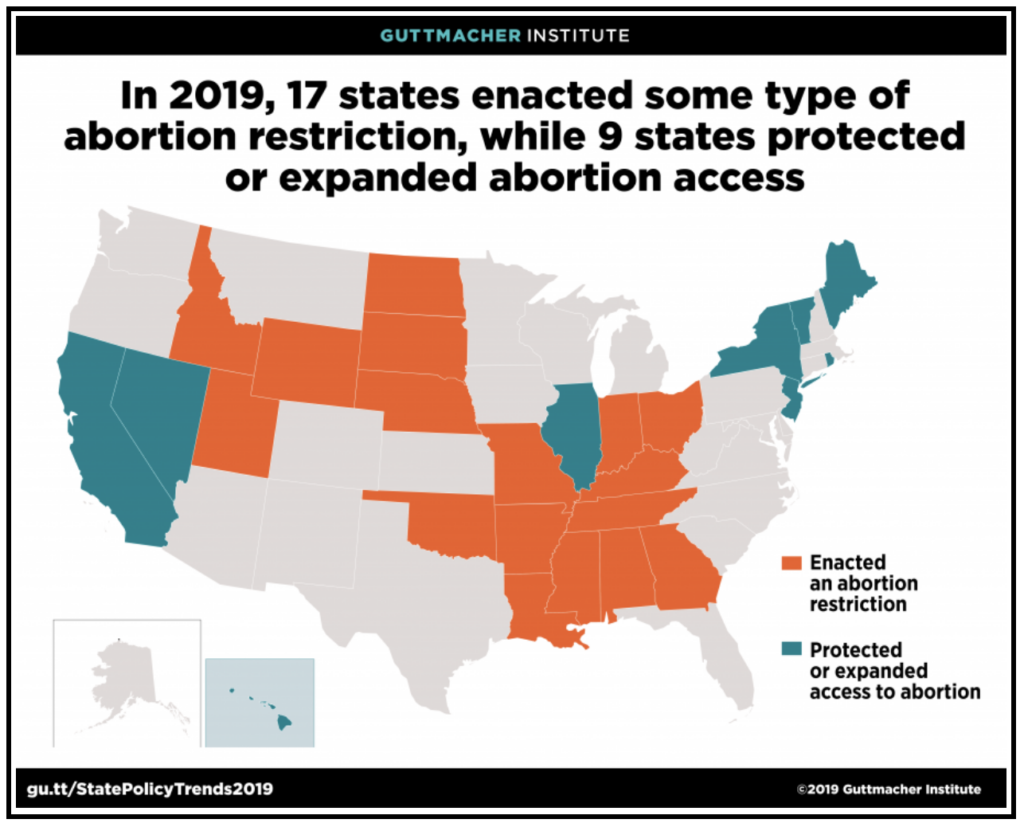
While 2019 saw a record number of abortion restrictions at the state level, it also saw more state abortion protections than in the entire decade prior. These included measures to protect abortion access, policies to decrease maternal mortality, and laws to increase access to contraception and to improve sex education. Equally important, governors in five states vetoed abortion restrictions.
Nearly 80 percent of state legislative seats are up for election this year. Efforts to elect pro-reproductive-rights legislators, along with governors and judges, will be crucial.
Enhancing gender diversity in our state legislatures is vital too. It’s no surprise that many of the states with the most draconian abortion laws also have the fewest women legislators in the nation (see Mississippi, Louisiana, Alabama and Kentucky). Races for district attorney and attorney general are also important, as they enforce and defend state laws.
U.S. Senate races in key states (like Maine, Alabama, Arizona, Colorado, Georgia, Montana and North Carolina) should be seen not only as pathways to federal judicial appointments, but also as openings for progressive legislation at the national level—like the Women’s Health Protection Act, which would provide a federal safeguard for the right to abortion.
Expanding our gaze even further, we have an opportunity and obligation to take a broader view of reproductive rights. The brutal killings of George Floyd, Breonna Taylor and so many other Black and brown people; the disproportionate impact of COVID-19 on communities of color; the caging of immigrants; and a broken public health care system have brought into sharp relief long-standing inequalities in this country. More Americans seem willing to acknowledge and support measures to address these injustices.

At the same time, abortion rights advocates have been pushing a broader and more inclusive reproductive justice agenda, including the EACH Woman Act to restore abortion coverage to Medicaid recipients (predictably, the bill has been stonewalled in the Senate). That agenda recognizes the outsize maternal and infant mortality rates among communities of color; the effect of domestic violence, bans on public funding of abortions, and the lack of paid leave; and other intersectional issues.
Lack of access to abortion rarely exists in a vacuum.
It’s no surprise, for example, that Louisiana has passed more abortion restrictions than any other state, while simultaneously having the second-highest maternal mortality rate in the country, with Black Louisiana women more than four times as likely to die in childbirth as white women.
COVID-19 has likewise presented a new lens through which to consider abortion rights. This global pandemic, made so much worse by the negligence and incompetence of the Trump administration, has forced many Americans to retreat to their homes. In the realm of health care delivery, this has meant an explosion in telemedicine.
Innovations in telemedicine, combined with the availability of medication abortion, hold enormous promise for the future of reproductive justice.
For so many women, the real barriers to access come in the form of travel, costs, hours and days off of work, lack of child care, overnight stays and the schedules of doctors who must fly in to provide care. That largely goes away with telemedicine.
Anti-abortion forces recognize the liberating impact of remote care and have worked hard to curb it (including 18 states that limit telemedicine for abortion and 12 states that have sought to exploit the pandemic to restrict abortion). Having experienced the virtues of telemedicine, Americans are unlikely to give it up so easily. And as it becomes more widespread, it will be harder to justify unequal treatment for abortion.
June Medical was an important win in the Supreme Court, particularly given what might have been. But it did not secure the right to abortion before this Court. Quite the opposite: It revealed a majority as poised as ever to undermine reproductive rights if given another chance.
While we don’t have the Supreme Court on our side and may not for a while, we have what we need to secure abortion rights for the future: a pro- reproductive-rights majority in an election year and a country tuned in to inequality.
You may also like:


