
To honor five-plus decades of feminist reporting, rebelling and truth-telling, From the Vault features some of our favorite classics from the pages of Ms. The complete Ms. Magazine Archive—every issue since 1972—is now available digitally on ProQuest: free to students, educators and activists via their libraries. Ask your local or campus librarian about subscriptions or free trial access. (More info here.) For an essential collection you can hold in your hands, don’t miss 50 YEARS OF Ms.: THE BEST OF THE PATHFINDING MAGAZINE THAT IGNITED A REVOLUTION (Alfred A. Knopf)—a stunning anthology of the most audacious, norm-breaking stories Ms. has published.
From the Winter 2018 issue of Ms.:
I couldn’t turn over in bed. My head would lift a bit, I could get part of a shoulder up, but even when I groaned with effort, my spine didn’t budge. My muscles weren’t responding to my brain’s requests.
My brain itself wasn’t functioning so well either. It felt swollen, as if it were trying to push out my eyeballs. Speaking required spearing the words one by one before they scampered out of my head. Thinking hurt, so mostly I didn’t do it, retreating into a twilight zone, alive but not living.
Until a year earlier, I’d managed to live a full if constrained life in spite of my decadelong illness. I’d applied every bit of determination I could muster to build my career as a science writer, to be a good partner, to hold on to my dreams and ambitions, despite getting stuck in bed unpredictably for days or weeks.
But now I was too sick to even care for myself. I had run out of medical treatments after going to the top specialists in the world.
Not only that, but I was running out of money, and I’d watched fellow patients repeatedly get turned down for disability payments. I felt as though I’d fallen off the edge of the earth.
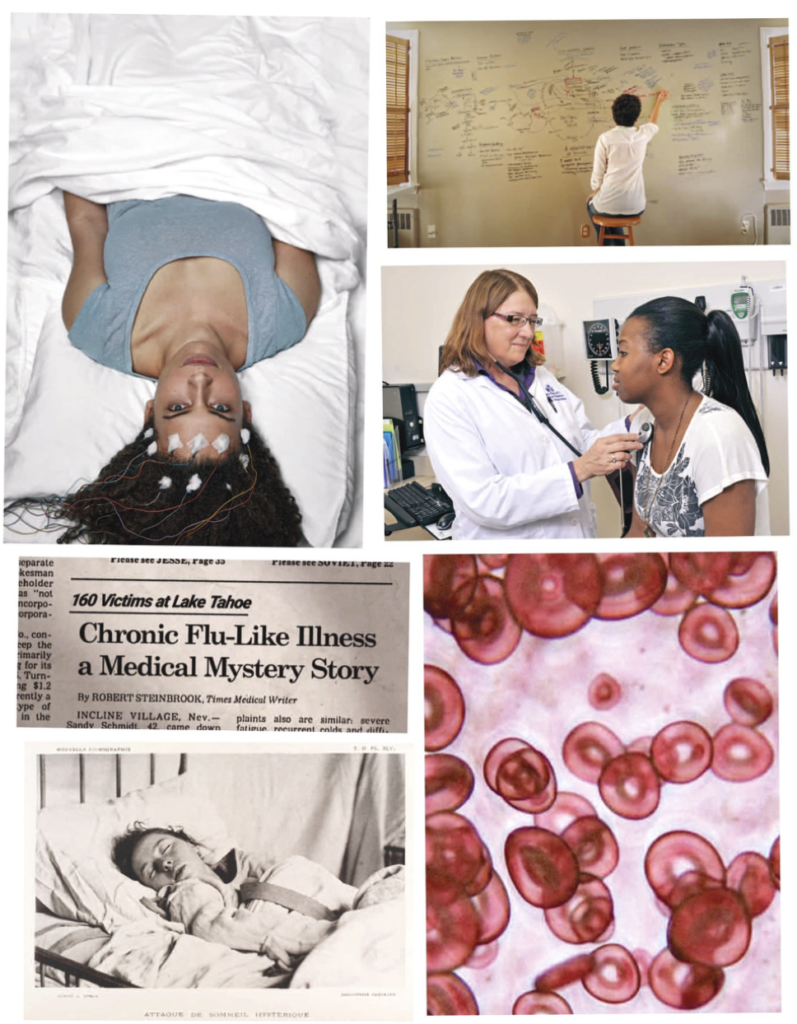
The very name of the illness that had so totally derailed my life sounded like a joke, as if it were nothing more than ordinary life in our too-fast age, the complaint of someone too lazy to keep up. The words stung my lips with insult: “chronic fatigue syndrome.”
Though I felt like I was suffering in my own private hell, more than a million Americans shared my fate. Worldwide, the number is estimated at between 17 and 30 million. Though the disease has been characterized as the “yuppie flu,” it is more common in poor people. It occurs in all racial groups and ages but most of us are women—around 80 percent.
Hidden in these numbers is astonishing suffering. Patients with chronic fatigue syndrome (CFS) have the lowest quality of life and greatest disability of any disease tested, including lung disease, rheumatoid arthritis and heart disease. A quarter of us are homebound. In 2014, a quarter of Canadian patients had less than $20,000 a year in income, and more than a quarter lived with food insecurity, the highest rate of any disease. Because CFS can disable people for decades, its economic impact is huge: In the U.S., it accounts for between $18 billion and $24 billion per year in medical costs and lost wages.
But public health agencies have treated chronic fatigue syndrome as if it were the jest the name suggests. The Centers for Disease Control and Prevention (CDC) chose and promulgated that insulting name even though internationally the disease is more commonly known as “myalgic encephalomyelitis” or ME—literally meaning “muscle pain and inflammation of the brain and spinal cord.”
The CDC then worsened its mistake by using absurdly broad definitions of the disease that include many people who are chronically tired but don’t have CFS at all, scrambling the research and confusing doctors. In particular, their definitions don’t require the hallmark symptom of the illness: Even slight exertion can exacerbate all the other symptoms of the disease. And medical schools rarely train doctors about ME/CFS at all, so few patients can get skillful medical care.
The very name of the illness that had so totally derailed my life sounded like a joke, as if it were nothing more than ordinary life in our too-fast age, the complaint of someone too lazy to keep up. The words stung my lips with insult: ‘chronic fatigue syndrome.’

Also, for years the National Institutes of Health (NIH) invested only $6 million a year in research on ME/CFS—six bucks a patient. To be comparable to other diseases with a similar impact, that budget would need to be $150 million or more.
In 2000, the disease was moved to the Office of Research on Women’s Health, even though some 200,000 men have the disease, and the funding dropped immediately and steadily. Contempt for the illness at the CDC was so great that even when the U.S. Congress set aside money for ME/CFS research in the 1980s, the agency used that money for other purposes—and then lied to Congress to cover it up.
Furthermore, much of the pitiful bit of research money has gone to scientifically flawed studies claiming that the disease was substantially psychological.
In 2011, the crown jewel of such studies was published in The Lancet and ballyhooed in the media worldwide: the $8 million British PACE trial, which claimed that psychotherapy and exercise could help or even cure CFS.
Psychotherapy and exercise became the worldwide standard of care, backed by recommendations from the CDC, the Mayo Clinic, Kaiser Permanente, UpToDate, the British National Health Service and many others. Those recommendations aren’t just useless but potentially dangerous, given that the chief symptom of the disease is that exertion can make patients worse.
“When I got into this, I was like, ‘Are you kidding me?’” said Mary Dimmock, a biochemist who retired from a 31-year career in research and development in the pharmaceutical industry after her son was disabled by ME/CFS. She became an advocate and wrote Thirty Years of Disdain: How HHS and a Group of Psychiatrists Buried Myalgic Encephalomyelitis.
“This isn’t science or medicine as I had come to know them,” she writes, “but rather a parade of psychogenic bias, neglect, bad science, flawed public policy and the political agendas of powerful people and institutions that have sentenced ME patients to the medical equivalent of the most squalid slum in the poorest country on earth.”
Carol Head, president of the Solve ME/CFS Initiative, likens the situation to the way that autism was once blamed on cold, unloving mothers. “I think similarly people will be ashamed of the views they had of ME/CFS in 2017,” she said. The dismissiveness arises partly, she said, because it is a genuinely complex illness that isn’t yet diagnosable with an objective test. But the stigma is also driven by the trivializing name—and the fact that it predominantly affects women.
The stigma began to develop not long after the CDC started investigating a mysterious and terrifying illness that swept through the Lake Tahoe area in the mid-1980s. Along with staggering, crushing fatigue, the patients (more women than men) experienced a bizarre multitude of extreme symptoms: dizziness, rashes, gut problems, hair loss, sensitivity to light, racing hearts, blurred vision, confusion, seizures. Some were paralyzed or unable to speak.
But after a perfunctory investigation, the CDC investigators grew skeptical. Though the illness was severe, patients’ lab results were pretty normal. Symptoms varied so much from one patient to the next that it was difficult to even come up with a working definition of the illness. In her definitive history of the disease, Osler’s Web, Hillary Johnson reported that the investigators quickly concluded that the only epidemic in Tahoe was an epidemic of diagnosis, not disease.
Eventually, local doctors gave patients less-common tests and found objective abnormalities. But by then, the CDC investigators’ attitude had curdled into scorn.
Under pressure, the CDC developed the first of its overly broad definitions of the disease. And it rechristened it, disregarding its similarities to myalgic encephalomyelitis. The name “chronic fatigue syndrome” might well have been designed to dismiss any concerns about its seriousness.
Around this time, unusual patients began appearing in the office of a young immunologist who specialized in AIDS cases, Dr. Nancy Klimas. They didn’t have HIV, but they were unimaginably exhausted. They were convinced something was wrong with their immune systems. Tests showed such a consistent set of immune abnormalities that Klimas became convinced they were suffering from some unidentified illness. She became their doctor, not just treating them but researching them in the lab and representing them to government health agencies. Klimas participated in the blossoming of worldwide research into HIV/AIDS, spurred by enormous investments from the NIH. Her HIV patients began to flourish with effective medications.
“Sadly, the ME/CFS field has had far less investment,” she said, “and my ME/CFS patients suffer, and I mean suffer, every day. If I had to have one or the other, I would rather have HIV than ME/CFS.”
Klimas’ decades of treating and researching the illness showed her that a series of triggers—a particularly bad virus, a toxic exposure, a trauma, or a combination of those and other physiological insults—send the immune system into overdrive. This leads to problems that have been documented in nearly every system of the body, including neuroinflammation, immune burnout, difficulty regulating blood pressure and heart rate when standing, out-of-whack hormones and problems with the mitochondria, the tiny power plants inside cells.
Currently, there are no FDA-approved treatments for ME/CFS, but Klimas works to address all of the patients’ symptoms at once. Sometimes, this is enough to push patients’ bodies back into a healthier state.
But few ME/CFS patients can access such care. There are very few specialists across the United States with Klimas’ level of experience, and she herself has had trouble getting young researcher-physicians interested in the disease because of the lack of research funding. Studying ME/CFS patients has looked to newcomers like “a career-killing move, because there was no money there,” she said.
Klimas also studies the better-funded Gulf War Illness, which affects veterans in ways that are symptomatically indistinguishable from ME/CFS. “I have to say that there’s a gender thing,” she said. “Three hundred thousand people, mostly men, are as sick as 1 million people, mostly women. And they have 10 times the research budget. What’s that about?”
And indeed, the mess that ME/CFS patients face is a potent distillation of problems that are rampant throughout women’s health. Women’s health activism has tended to focus on our girl parts, but discrimination affects our entire bodies. Sick women are remaining undiagnosed and untreated, for a tangle of reasons with sexism at the core.

Research in illnesses primarily affecting women tends to be underfunded relative to their disease burden, and doctors get minimal education about them. When illnesses affect both sexes, their impacts on men are often better-understood than those on women. Women suffering heart attacks, for example, commonly get misdiagnosed because doctors only look for the crushing chest pain more common in men, disregarding the gut pain and sweating more common in women. Until 1993, women were excluded from clinical trials entirely, even though many drugs affect us differently, leaving a continuing hole in our knowledge.
In the past few years, extraordinary efforts throughout the ME/CFS community have brought some remarkable changes. Head’s organization, the Solve ME/CFS Initiative (SMCI), has leveraged its own modest budget to achieve disproportionate research progress and has pressured the government to dramatically increase research funding. Along with leading groundbreaking studies of its own, it has funded early-stage research to enable new scientists in the field to get the foundational results they can use to get larger grants elsewhere.
When health agencies for years ignored calls for a national registry of patients for research—a foundational need for any illness—SMCI stepped into the gap and started one. And after Congress zeroed out the CDC’s research budget for ME/CFS each of the past several years, SMCI, working with other advocates, convinced it to restore the funding. SMCI also led the organization of 80 meetings between patients and congressional representatives on one day in 2016, in collaboration with the patient organization #MEAction.
Women’s health activism has tended to focus on our girl parts, but discrimination affects our entire bodies. Sick women are remaining undiagnosed and untreated, for a tangle of reasons with sexism at the core.
All these efforts have at last brought action from public health agencies. In 2015, the prestigious National Academy of Medicine (then called the Institute of Medicine) wrote a report reviewing the research on ME/CFS and concluding it is “a serious, chronic, complex, systemic disease that frequently and dramatically limits the activities of affected patients.” The report also emphasized that chronic fatigue syndrome is distinct from chronic fatigue and that the key sign of the disease is the inability to tolerate exertion, not tiredness.
A few months after this, following a powerful open letter from a patient, the NIH announced that it would increase research funding and perform an in depth study of ME/CFS itself.
“Given the seriousness of the condition,” said NIH director Francis Collins in an interview with The Atlantic, “I don’t think we have focused enough of our attention on this.”
The NIH recently funded four projects through a pot of $7 million that it set aside for the illness. Funding is still pathetic—it’s slated to be $13 million in 2017—but at least we have the NIH’s attention.
Also, top-notch researchers have gotten interested in the disease and started producing striking findings showing abnormalities in metabolism and immune function, among other problems. Journalist David Tuller exposed the problems with the PACE trial of psychotherapy and exercise that patients had been pointing out for years, and he rallied the scientific community against it. This pressure forced the CDC to finally remove its recommendation of the treatments on its website. And the once-abysmal quality of journalism about the disease overall has improved substantially. Klimas has developed a treatment she’s ready to send into clinical trials. “It’s a time of hope,” she said.
Up next:
U.S. democracy is at a dangerous inflection point—from the demise of abortion rights, to a lack of pay equity and parental leave, to skyrocketing maternal mortality, and attacks on trans health. Left unchecked, these crises will lead to wider gaps in political participation and representation. For 50 years, Ms. has been forging feminist journalism—reporting, rebelling and truth-telling from the front-lines, championing the Equal Rights Amendment, and centering the stories of those most impacted. With all that’s at stake for equality, we are redoubling our commitment for the next 50 years. In turn, we need your help, Support Ms. today with a donation—any amount that is meaningful to you. For as little as $5 each month, you’ll receive the print magazine along with our e-newsletters, action alerts, and invitations to Ms. Studios events and podcasts. We are grateful for your loyalty and ferocity.


