
Abortion is a very common procedure—one in four U.S. women will have one—yet most people still know so little about it.

After reading about Kate Cox’s unsuccessful efforts to obtain an abortion in Texas, I needed an outlet for my ire. I took to social media, where I found reprehensible comments about abortion on Threads. I responded to them. I schooled my interlocutors with facts and links to research. I dazzled them with my correct grammar. I received tens of likes.
You may be shocked to learn that I changed no one’s mind. I was nevertheless surprised by some people’s misconceptions about abortion—many of which appeared to be shared by pro- and anti-abortion individuals.
For example, people seemed unaware that most individuals who seek abortion care were using contraception when they became pregnant.
Some of the misconceptions that I read, especially those about the safety of abortion procedures, have been comprehensively addressed elsewhere, but others have not. Abortion is a very common procedure—one in four U.S. women will have an abortion by the time she reaches age 45—yet most people still know so little about it.
In the spirit of clearing the cobwebs out of our collective discourse, here are a few facts about abortion that have not been widely reported.
1. Most people who obtain abortion care in America report using contraception in the month in which they became pregnant.
“Many people think abortion is used as a primary form of birth control, but that is incorrect,” said Dr. Daniel Skora, a fertility specialist in Texas.
Data confirm this point.
- A slim majority of abortion patients (51 percent in 2014, and 54 percent in 2000) in the United States reported that they used contraception in the month in which they became pregnant, according to the Guttmacher Institute.
- The most common form of contraception was the condom (28 percent and 24 percent in 2000 and 2014, respectively).
- The second most common form was the pill (14 percent and 13 percent in 2000 and 2014, respectively).
Although long-acting reversible contraceptive methods, such as intrauterine devices (IUDs) and contraceptive implants, are over 99 percent effective at preventing pregnancy, people using these methods can still become pregnant.
In other words, even the best-laid contraceptive plans do not eliminate the need for abortion care.
2. Most people who obtain abortion care in America are already parents.
CDC data show that 60 percent of people who receive an abortion already have at least one child. Many of these people indicate that they are seeking abortion care because they want to be able to care for their existing children better than they could with an additional child in the family.
3. Most people who obtain an abortion in America are religious.
Roughly 60 percent of Americans who have an abortion identify as religious. The largest fraction (24 percent) of these believers identify as Catholic, while 17 percent are mainline Protestant, and 13 percent are evangelical Christians. The remaining 8 percent of the believers report some other affiliation. Around 38 percent of abortion recipients do not identify as religious.
4. Around 16 percent of people who seek abortion care in America identify as LGBTQ+.
Roughly 16 percent of people who sought abortion care between June 2021 and July 2022 did not identify as heterosexual, according to a survey by the Guttmacher Institute.
In the same period, 1.1 percent of people who sought abortion care did not identify as female.
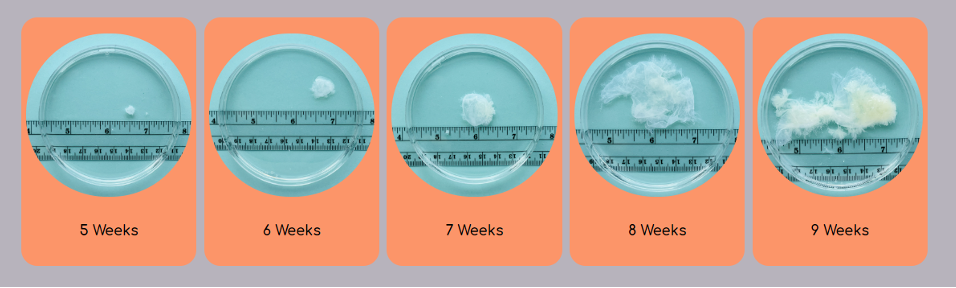
5. Many fetal anomalies cannot be detected until after the first trimester.
Most people in America have mixed views about abortion. That is, they believe that abortion should be legal, but not in all circumstances. Many people who hold this view would prefer to limit abortion access to the first trimester, which runs from roughly week zero to week 13 of pregnancy (as measured from the date of the pregnant person’s last menstrual period).
But there are all sorts of reasons why a person may be unable to terminate a pregnancy during the first trimester. They may not realize that they are pregnant because their periods are irregular. They may struggle to find the financial resources necessary to obtain an abortion. They may be unable to take time off work. They may need time to find someone to watch their children while they schedule and attend visits to the doctor.
Even if the pregnancy is planned and wanted, a person may need to terminate because of a fetal anomaly—but fetal anomalies typically cannot be definitively diagnosed during the first trimester.
“I really wish that people knew that it takes a really long time to know that something is wrong,” Dr. Mahino Talib, an OB-GYN on the faculty at NYU, told me. “And even when someone does all the tests and makes the hard decision to terminate the pregnancy, it takes a long time to schedule the procedure, including in major cities like New York.”
Even with access to the best medical care, pregnant people typically receive only one ultrasound and one set of blood tests in the first trimester. These tests can indicate the presence of a fetal anomaly, but they cannot conclusively diagnose it. At this point in the pregnancy, the fetus is not developed enough for many structural abnormalities to be seen on the ultrasound. And the blood tests done at this stage have not been validated as a means to diagnose most genetic anomalies.
I really wish that people knew that it takes a really long time to know that something is wrong.
Dr. Mahino Talib, OB-GYN
If initial tests do indicate an anomaly, virtually all pregnant people pursue other testing to confirm the diagnosis—which means further delay. The two options for confirmatory tests are chorionic villus sampling, which is typically done between 12 and 14 weeks of pregnancy, and amniocentesis, which is done after roughly 15 weeks. Obtaining full results from these tests routinely takes a week. In other words, even if tests done during the first trimester indicate an anomaly, confirmatory testing typically pushes a pregnancy into the second trimester.
And that is the best-case scenario. Many pregnant people, especially those who live in areas that are under-resourced in terms of maternal medicine providers, do not receive all or any of these tests. For them, the first time they may become aware of an anomaly is when they receive an ultrasound around 20 weeks. The majority of structural abnormalities—including fatal brain and heart abnormalities—are not detected until this ultrasound because the fetus must be sufficiently developed for those anomalies to be apparent.
Once an anomaly is definitively identified, a pregnant person then needs additional time to process the information, make a decision about how to proceed, and schedule the procedure—all of which means that limiting abortion access to the first trimester makes little sense.
6. Several prisons and jails do not allow any abortion access for incarcerated individuals.
Even before the Supreme Court reversed Roe v. Wade, prisons and jails had a spotty record of helping pregnant incarcerated people access abortion care. A one-year analysis spanning 2016 to 2017 found that 14 percent of state prisons did not allow abortion at all. Many other facilities required people seeking abortion care to pay the full cost of the procedure—a rule that effectively foreclosed access to abortion for many.
Although data about incarcerated people seeking abortion care since the reversal of Roe are not yet available, even greater numbers of these individuals are likely to be denied access to the care they need now.

No matter what you think about abortion access, it helps to understand the realities of someone facing the decision of whether to terminate.
“It is really easy to say you condemn abortion when you have never met someone who has had one.” Dr. Talib said. “I have been doing this for a long time, since 2013, and I have never met a single patient who went forward with a pregnancy termination who did not have an emotional discourse about it.”
If you do oppose abortion rights, there is one more thing you should know: Banning the procedure is not the best way to achieve your desired ends. Abortion restrictions do not lower abortion rates; they only make abortion less safe.
“The most important thing the country can do to lower the abortion rate is increasing access to pregnancy healthcare, contraception and education,” Dr. Skora said.
Anti-choice advocates should do those things if they want to have a leg to stand on in the ongoing abortion debate.
Up next:
U.S. democracy is at a dangerous inflection point—from the demise of abortion rights, to a lack of pay equity and parental leave, to skyrocketing maternal mortality, and attacks on trans health. Left unchecked, these crises will lead to wider gaps in political participation and representation. For 50 years, Ms. has been forging feminist journalism—reporting, rebelling and truth-telling from the front-lines, championing the Equal Rights Amendment, and centering the stories of those most impacted. With all that’s at stake for equality, we are redoubling our commitment for the next 50 years. In turn, we need your help, Support Ms. today with a donation—any amount that is meaningful to you. For as little as $5 each month, you’ll receive the print magazine along with our e-newsletters, action alerts, and invitations to Ms. Studios events and podcasts. We are grateful for your loyalty and ferocity.


