
Updated Monday, June 24, at 10:15 a.m. PT.

A decision from the U.S. Supreme Court will be coming any day now in two cases, Idaho v. United States and Moyle v. United States, about whether states can prohibit doctors from treating women with life-threatening pregnancies until a patient’s condition deteriorates to the point where they are about to die.
The National Women’s Law Center (NWLC) filed an amicus brief in these cases describing several of the more than 70 documented cases of women almost dying—and at least one who did die—when they were denied emergency medical care because of abortion bans enacted across the country after the Supreme Court overturned Roe v. Wade in June 2022. And “the true number of cases is likely significantly higher,” according the NWLC brief.
In these cases, the Department of Justice (DOJ) is challenging Idaho’s “Defense of Life Act,” which prohibits abortions unless necessary to save the life of the mother. The DOJ argued that Idaho’s law violates the federal Emergency Medical Treatment and Labor Act (EMTALA), which requires Medicaid-funded hospitals to provide medically necessary stabilizing treatment to patients, including pregnancy termination, regardless of state laws restricting or banning abortion. The DOJ argued doctors violate federal law if they wait until a patient’s condition deteriorates to the point where they are about to die before doctors provide the necessary care to stabilize them.
Federal law requires federally funded hospitals to provide “necessary stabilizing treatment” to any patient with an emergency medical condition that, in the absence of medical attention, could reasonably be expected to result in putting a patient’s health in serious jeopardy, including “serious impairment of bodily functions or serious dysfunction of any bodily organ or part.”
The Idaho law prohibits treatment until a woman is on the brink of death, without regard to the impacts on her health otherwise.
“It’s not harmless to wait until the brink of death to intervene in emergency medicine,” said emergency room physician Dr. Dara Kass at Columbia University Medical Center. “Having to wait until that window to intervene is dangerous for people… [and] will have consequences to your life and future fertility and organs and a lot of other things.”
Oral Arguments Overview
On April 24, the Supreme Court held two hours of oral arguments on whether states can require women to sacrifice their health and well-being in order to continue nonviable pregnancies.
Idaho’s attorney Joshua Turner argued that women experiencing pregnancy complications have no federal right to medical care unless they are dying. Justices Samuel Alito and Clarence Thomas clearly agreed, and Justices Neil Gorsuch and Brett Kavanaugh also appeared to agree. These five men expressed utter disregard for women’s lives and dignity.
The bipartisan group of women on the Court were the only ones asking questions reflecting concern about the impact of the decision on women’s lives and health—demonstrating the importance of having women on the Court.
Chief Justice John Roberts said hardly anything.
NWLC Brief: Harrowing Stories of Denied Emergency Medical Care
The National Women’s Law Center brief detailed the excruciating stories of several pregnant women denied emergency medical care, demonstrating the harms of such denials.
One involved a woman experiencing preterm premature rupture of membranes (PPROM), which is when the amniotic sac or “water” breaks prior to 37 weeks. PPROM complicates 2 to 4 percent of all singleton pregnancies and 7 to 20 percent of twin pregnancies, and impacts 150,000 women in the U.S. every year. In states banning abortion, women experiencing PPROM face life-threatening dangers.
The NWLC brief outlined:
One patient experienced PPROM before her fetus was viable. The stabilizing treatment for pre-viable PPROM may be terminating a patient’s pregnancy, either through an induction of labor or a dilation and evacuation (D&E)—a routine procedure. But this patient was sent home without that care. She returned to the emergency room two days later with severe sepsis and bacteremia.
Her pre-viable fetus was delivered, but clinicians could not deliver her placenta. Eventually, a physician performed a D&E, but unlike healthy patients, this woman bled “from everywhere.” The patient miraculously lived, but after her gut-wrenching experience, the concern she expressed to her doctor was whether her severe infection “count[ed] as life-threatening,” or whether she and her doctor would “go to jail” for the procedure that saved her life.
Another story involved hospital anesthesiologists, who refused to provide an epidural to a woman in early labor because he feared criminal prosecution:
Another patient in an abortion ban state sought treatment for a dilated cervix, through which her amniotic sac was protruding, when she was 19 to 20 weeks pregnant. She was sent home.
The following day, she came to the emergency department in severe pain and advanced labor. While EMTALA requires stabilizing treatment for pain and stabilizing care during labor, the hospital’s anesthesiologists refused to provide an epidural.
As the patient’s physician described:
“[The anesthesiologists] believed that providing an epidural could be considered [a crime] under the new [state] law. The patient received some IV morphine instead and delivered a few hours later but was very uncomfortable through the remainder of her labor. … I overheard the primary provider say to a nurse that so much as offering a helping hand to a patient getting onto the gurney while in the throes of a miscarriage could be construed as ‘aiding and abetting an abortion.’ Best not to so much as touch the patient who is miscarrying…”
Denial of emergency care not only endangers the lives and health of pregnant women, but can cause devastating financial impacts—including the costs of traveling out of state to obtain emergency treatment, lack of insurance coverage for out-of-state care, and absence from work, which can endanger employment status.
These impacts are particularly burdensome to low-income patients and their families:
Mylissa Farmer was denied the emergency abortion care she needed, first by her local hospital in Missouri, and then by a hospital in Kansas. After diagnosing her with PPROM, doctors at both hospitals told Mylissa her fetus could not survive, and continuing her pregnancy would put her at risk of serious infection, hemorrhaging, the loss of her uterus, and even death.
Still, both hospitals refused to end the pregnancy, in violation of EMTALA. With her health deteriorating rapidly, Mylissa and her boyfriend drove more than four hours to an Illinois abortion clinic while she was in labor.
The medical and financial consequences of crisscrossing state lines to obtain life-saving abortion care linger to this day. Mylissa was docked pay for missing work and had to raise funds to pay for the Illinois care that her insurance refused to cover. Her boyfriend also lost his job because he was forced to miss work over the days he helped her travel. They could not regain steady employment for months.
Yeniifer Alvarez’s Story
Some women never get the care they need. The NWLC brief details the case of one young woman, Yeniifer (Yeni) Alvarez, who died from pregnancy complications after a Catholic hospital in Texas failed to offer stabilizing abortion care.
Yeni lived in an immigrant community in Luling, Texas, where 65 percent of residents lack health insurance—Yeni included. She learned she had hypertension and diabetes during her pregnancy, and developed pulmonary edema at the height of the COVID-19 pandemic. Because she was uninsured, she was unable to afford the care and medications needed. As her condition deteriorated, she went to the emergency room multiple times, but doctors did not offer abortion care.
Experts agree that Yeni’s death likely could have been prevented with an abortion, but hospital records show that, despite multiple emergency room visits (including one where she was struggling to breathe), healthcare providers never offered to end her pregnancy.
Yeni’s death represents what the lack of access to healthcare can mean for a pregnant person marginalized by lack of health insurance, poverty, and a draconian abortion ban.
As Yeni’s family mourn her preventable death, her loss has led to serious financial and familial hardship because Yeni contributed to the mortgage payments and was a frequent caregiver for a cousin and an autistic sibling.
How Abortion Bans Harm Reproductive Healthcare Access Overall
Pregnancy in the United States is now 10 times more lethal than in other high-income countries, the National Women’s Law Center points out. Pregnant Indigenous women die twice as often as white women, while Black women die three times as often as white women.
States restricting abortion have much higher maternal mortality rates than states with abortion access. In 2020, restrictive states had a 62 percent higher maternal death rate than other states, and experts estimate that total abortion bans today are causing a nearly 25 percent increase in maternal mortality overall.
One third of counties in the United States are “maternity care deserts,” with no obstetric providers, hospital-based obstetric care or birth centers. And Dobbs has worsened this dearth of providers.
In the first 15 months after enacting an abortion ban, Idaho—the state at the heart of the EMTALA case in front of the Court—lost 22 percent of its practicing obstetricians and 55 percent of its high-risk obstetricians. At least two Idaho hospitals closed their labor and delivery units in 2023.
Obstetric providers are moving away from states where they cannot save their patients’ lives and health without the looming threats of imprisonment, bankrupting civil penalties and losing their medical licenses.
“With fewer providers, all pregnant people, especially Black and Indigenous people, will suffer life-changing harms, and many will die preventable deaths,” argued the NWLC brief.
One third of counties in the United States are ‘maternity care deserts,’ with no obstetric providers, hospital-based obstetric care or birth centers. And Dobbs has worsened this dearth of providers.
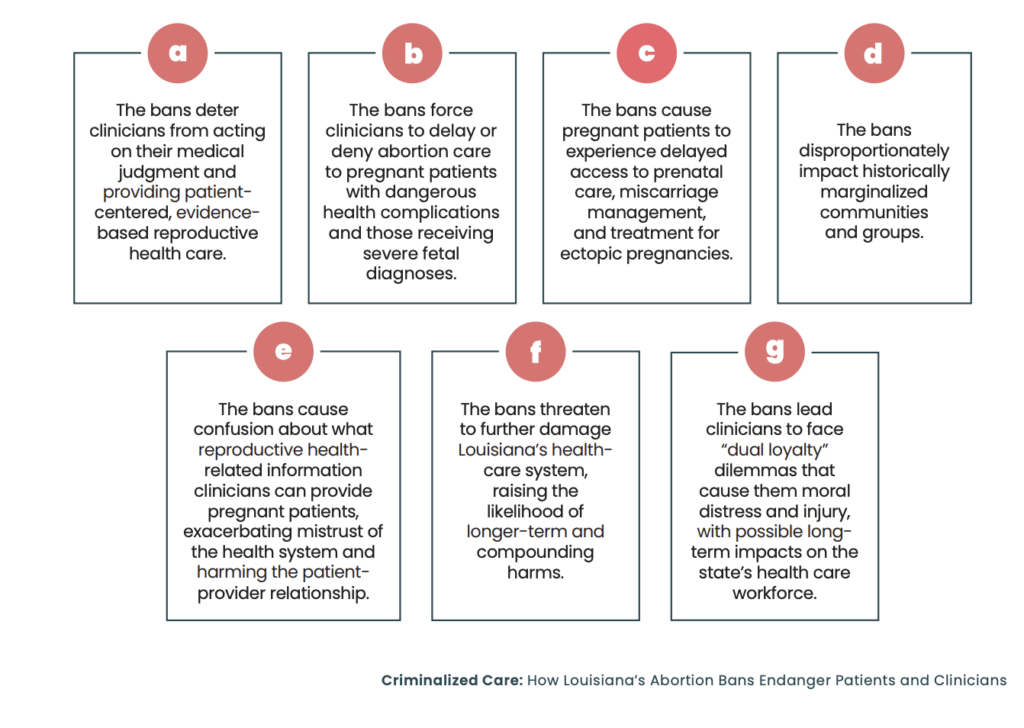
Louisiana’s abortion ban is endangering the lives of women needing emergency medical care for pregnancy complications, as shown by a recent report, “Criminalized Care: How Louisiana’s Abortion Bans Endanger Patients and Clinicians,” by Lift Louisiana, Physicians for Human Rights, RH Impact and the Center for Reproductive Rights.
It also documented how some doctors in Louisiana are doing medically unnecessary and dangerous cesarean sections instead of safe abortions due to fears of violating the law.
“The bans’ narrow and ill-defined exceptions create confusion, uncertainty and fear for both pregnant patients and clinicians, who face significant professional, civil and criminal penalties for providing the patient-centered and compassionate care they were trained for and could legally offer before Roe v. Wade was overturned,” according to the report.
EMTALA and the Need for Clarification
In addition to the federal government’s attempts to enforce EMTALA, the Center for Reproductive Rights (CRR) has filed lawsuits in Tennessee, Oklahoma and Idaho asking states to clarify whether doctors can offer emergency medical care to pregnant patients experiencing complications, sharing many harrowing stories of pregnant women and their doctors.
On May 31, the Texas Supreme Court issued a devastating ruling in a parallel case, Zurawski v. Texas, rejecting the most significant challenge to Texas’ new abortion laws yet and ruling that the medical exceptions in the state’s anti-abortion laws were broad enough to withstand constitutional challenge.
Confusing language and non-medical terminology in the law has left doctors uncertain about when they are legally able to provide abortion care without being prosecuted.
Center for Reproductive Rights
In the Tennessee case, Blackmon v. Tennessee, the Center for Reproductive Rights is asking a court to clarify what circumstances qualify under the “medical emergency” exception in Tennessee’s abortion ban. CRR filed the case on behalf of nine plaintiffs: seven Tennessee women denied medically necessary abortion care who faced severe and dangerous pregnancy complications, and two Tennessee physicians who have been prevented from offering their patients the medically indicated treatment during obstetrical emergencies.

“Confusing language and non-medical terminology in the law has left doctors uncertain about when they are legally able to provide abortion care without being prosecuted,” argued CRR.
Doctors in the state face loss of licensure and up to 15 years in prison for violating the law, while the law forces pregnant women to either wait until they are near death to receive care or flee the state if they have the means to do so.
The Center for Reproductive Rights Takes on Tennessee’s Abortion Ban
The following stories, excerpted from The Center for Reproductive Rights, are some of the stories from pregnant women in Tennessee whose lives were put at risk due to delayed or denied abortion care.
Nicole Blackmon

Nicole Blackmon discovered she was pregnant just months after the murder of her teenage son. But at 15 weeks, her baby was diagnosed with a condition that made it unlikely her baby would survive the pregnancy. In addition to suffering from depression and anxiety, Nicole had health conditions that put her at high risk of having a stroke during labor and delivery. Without resources to travel to another state for an abortion, Nicole was forced to continue the pregnancy against her will until, at 31 weeks, she gave birth to a stillborn baby.
Allie Phillips

Allie Phillips was 18 weeks pregnant when she learned that her baby had multiple fetal diagnoses that made it unlikely her baby would survive the pregnancy, including a congenital condition of the brain. The continuation of the pregnancy posed risks to Allie’s own health. Allie was able to raise the funds to travel to New York City, where she learned her baby had already died in utero, leaving her at a high risk of infection and blood clots. She was able to receive the abortion care she needed in New York.
Katy Dulong
Katy Dulong was diagnosed with cervical insufficiency early in her second trimester and told that she would inevitably lose the pregnancy. Though she asked to receive abortion medication to expel the pregnancy, she was instead sent home. Katy did not receive the abortion care she needed until 10 days later—when her cervix was fully dilated, all amniotic fluid had drained, and most of the fetus’ body was in her vaginal canal. Katy’s doctors told her she was extremely lucky to have survived; without the abortion medication, she could have died within days.
Rebecca Milner
Rebecca Milner was 20 weeks pregnant when she learned she had suffered pre-term premature rupture of membranes (PPROM) and her baby was unlikely to survive. Continuing the pregnancy put her at risk of potentially life-threatening infection. She was able to travel to Virginia to obtain the abortion she needed. However, Rebecca still developed an infection that doctors said resulted from the delay in abortion care and needed emergency treatment for sepsis when she returned to Tennessee.
Rachel Fulton
Rachel Fulton learned from an ultrasound that her baby showed inadequate fetal development of the nervous system, lower spine, lungs, abdomen, feet, and hands, as well as fluid buildup in tissues and organs. The pregnancy was unlikely to survive to birth or long past birth, and continuing the pregnancy put Rachel at risk of developing mirror syndrome, a life-threatening complication. Rachel’s grandmother had died in childbirth, a tragedy that had a lifelong effect on Rachel’s father and his siblings. To safeguard her health and spare her family from such tragedy, she drove with her husband to Illinois to obtain abortion care.
Monica Kelly
Monica Kelly was 12 weeks pregnant when her doctor told her that her pregnancy had Trisomy 13, a severe fetal condition, and was unlikely to survive to birth or would die shortly after birth. Monica’s doctor warned her that continuing the pregnancy would put her at risk for preeclampsia and infection, among other conditions. Monica traveled to Florida to receive the abortion care she needed.
Kathryn Archer
Kathryn Archer was 20 weeks pregnant when she learned that several severe fetal conditions, including irregular brain development and improperly developed organs, made it unlikely that her pregnancy would survive to birth. After struggling to find an appointment out of state, Kathryn obtained abortion care in Washington, D.C.
Center for Reproductive Rights Intervene on Behalf of Idaho Women
CRR’s Idaho plaintiffs have similarly harrowing stories of near-death experiences while pregnant.
Jennifer Adkins

Lead plaintiff in the case Jennifer Adkins, of Caldwell, was pregnant with her second child when her 12-week ultrasound revealed her baby had skin edema and cystic hygroma, both of which carry a high mortality rate. During the same appointment, a geneticist told Jennifer that her daughter was also likely to have Turner syndrome, a rare chromosomal condition that affects female fetuses and results when one of the X chromosomes is missing. Doctors told Jen her pregnancy was likely not viable, as Turner syndrome almost always results in miscarriage. They also said that if she did not miscarry, Jen was likely to develop mirror syndrome—a condition leading to the development of edema and preeclampsia which, if left untreated, could be fatal.
Though Jennifer was devastated by the news, it was clear to her that continuing the pregnancy would endanger her health. Aware of Idaho’s abortion ban, she questioned her doctors, who admitted that if the state’s laws were different, they would have referred her to an in-state abortion clinic. But because of Idaho’s abortion laws, she would instead have to travel outside Idaho to get the care she needed. After calling several clinics in neighboring states, Jen was able to travel with her husband to Portland, Oregon, to obtain abortion care—but only after receiving financial assistance from two abortion funds. Later, Jen was able to get her fetal tissue tested, and the diagnosis of Turner syndrome was confirmed.
While Jen hopes to become pregnant again, she is anxious about being pregnant in Idaho. She worries that because her hospital has recently lost its obstetric genetics counselor and will soon lose its only remaining maternal fetal medicine (MFM) specialist, she will be left with little to no in-state options for genetic counseling and high-risk pregnancy care should she need it in future pregnancies.
Kayla Smith

Kayla Smith, formerly of Nampa, pregnant with her second child, was shocked to learn at her 19-week ultrasound scan that her baby had a serious and inoperable congenital heart condition. After consulting with a maternal fetal medicine (MFM) specialist and a pediatric cardiologist, she and her husband learned that their baby was not likely to survive past birth and there were no viable medical interventions available. Kayla’s doctors also explained that because Kayla had previously developed preeclampsia during her first pregnancy (her daughter is now 3), she had a heightened risk of developing preeclampsia again if she carried her pregnancy to term.
Devastated by the news but determined to spare their baby from suffering and ensure Kayla’s safety and health, Kayla and her husband decided that what Kayla needed was abortion care. But because of Idaho’s abortion bans, her doctors could not provide that care for her. Kayla and her family traveled to Washington to obtain abortion care—a trip that cost thousands of dollars and required them to take out a personal loan, as well as receive assistance from friends and family. Worse than the financial toll, Kayla was upset that she had been forced through such an ordeal just to obtain necessary medical care.
Kayla is pregnant again, with a girl—but she and her husband were so concerned about raising two daughters in a state like Idaho, where their bodily autonomy rights are not guaranteed or protected, that they have since moved to Washington.
Rebecca Vincen-Brown

Rebecca Vincen-Brown, of Ada County, was thrilled to be pregnant with her second child when she began experiencing vaginal bleeding approximately 12 weeks into her pregnancy. She had several ultrasounds and appointments with her obstetrician-gynecologist (OB-GYN) and MFM because her baby was measuring small and low in her uterus. After she underwent two rounds of non-invasive prenatal testing—which were inconclusive but showed a likelihood of severe chromosomal conditions—she went in for an early anatomy scan at 16 weeks and learned her baby had a number of fatal fetal conditions including dangling choroid plexus, micrognathia, significant cardiac issues and horseshoe kidney. Doctors told her the baby was unlikely to survive to birth, and if Rebecca were to continue her pregnancy, she risked developing preeclampsia or severe hemorrhaging.
Rebecca wanted to prevent her baby from suffering and remain healthy and present for her 2-year-old daughter, but her doctors were not able to provide her the care she needed due to the abortion bans. So she, her husband and their daughter drove for seven hours to Oregon so that she could obtain abortion care. After Rebecca had gone to the abortion clinic for the first day of her abortion procedure, she passed her pregnancy in the hotel bathroom in the early hours of the next morning. Her husband had to perform multiple rounds of fundal massage on her stomach to help stop the bleeding. They both had to be careful not to make any noise while their daughter slept.
Rebecca is pregnant again and recently learned she is carrying a baby girl. While happy to be pregnant, she is anxious about her health while pregnant in Idaho and is concerned about her daughters’ rights and safety.
Moving Ahead, Will the Court Allow Women to Die?
As Republican lawmakers and judges impose draconian abortion bans in more states, more pregnant women are suffering and dying, especially women of color and low-income women and women of color.
“We have never seen legislators look at the idea of intervening to prevent harm to somebody as then limited in its practice, but not for medical knowledge, not for changes in safety and efficacy, but only because legislation has decided that that procedure is only allowable in certain circumstances,” said Dr. Dara Kass.
Will the Supreme Court allow women to die?
*
For more Dobbs survivor stories, visit the website of the Center for Reproductive Rights, including Voices from Abortion Ban States and stories of the plaintiffs in Zurawski v. Texas, Cox v. Texas, and the Idaho, Tennessee and Oklahoma cases. Here’s a CRR press conference with patients speaking out. CRR features the stories of plaintiffs in cases against Idaho, Tennessee and Oklahoma here.
The Center for American Progress has a provider storyteller series, featuring four medical professionals from Idaho and other rural states testifying about how the criminalization of abortion care and the interference of the Supreme Court in their daily medical practice has changed their personal and professional lives.
The Ms. series “Our Abortion Stories” also chronicles readers’ experiences of abortion pre- and post-Roe. Share your abortion story by emailing myabortionstory@msmagazine.com.
Up next:
U.S. democracy is at a dangerous inflection point—from the demise of abortion rights, to a lack of pay equity and parental leave, to skyrocketing maternal mortality, and attacks on trans health. Left unchecked, these crises will lead to wider gaps in political participation and representation. For 50 years, Ms. has been forging feminist journalism—reporting, rebelling and truth-telling from the front-lines, championing the Equal Rights Amendment, and centering the stories of those most impacted. With all that’s at stake for equality, we are redoubling our commitment for the next 50 years. In turn, we need your help, Support Ms. today with a donation—any amount that is meaningful to you. For as little as $5 each month, you’ll receive the print magazine along with our e-newsletters, action alerts, and invitations to Ms. Studios events and podcasts. We are grateful for your loyalty and ferocity.


