

The Pregnant Worker Fairness Act (PWFA) went into effect this summer. Perimenopause and menopause are related to workers’ reproductive lives and capacity for pregnancy. The inclusion of these terms will provide valuable guidance to employers and the millions of affected workers.
Tag: Medical Sexism

The First Tool to Name Obstetric Racism Might Finally Push Policymakers Into Action
Awareness of the U.S. maternal health crisis has increased—but a parallel crisis of human rights violations against pregnant and postpartum people remains invisible or misunderstood. By convening two People’s Tribunals to End Obstetric Violence and Obstetric Racism before the end of the year, we aim to change that. The first will happen on Oct. 6 in New York City at the NYU Law School, and the second on Dec. 1 in Memphis, at BRIDGES USA.
We cannot fix the maternal mortality problem without fixing the human rights problem at its core.
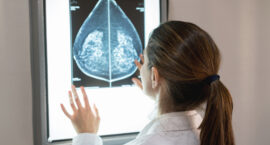
We Need More Awareness and Research on Benign Breast Conditions
The most common benign breast tumor is called a fibroadenoma. It is estimated to impact one in four women overall. Despite its frequency, most people have never even heard the term.
We need more research and awareness, starting a larger conversation about women’s health, cancer risk factors and quality of life.
‘Women’s Pain Is Less Important’: Documentary ‘Below the Belt’ Shows Why Endometriosis Is a Feminist Issue
A new documentary Below the Belt, executive produced by Hillary Clinton and directed by Shannon Cohn, demonstrates why endometriosis—and women’s health—is an urgent social justice issue for feminists.
The film follows the lives of four women living with endometriosis—a disease that can cause debilitating pain, infertility and menstrual issues.

The Price of Gender Bias
In male-dominated fields, women continue to be undervalued in the workplace. A male standard is the default in fields built by men for men.

‘They Decriminalized Abortion, But They Still Judge Us’: The Mexican Fight for Reproductive Justice
In the case of abortion, which the supreme court decriminalized in September 2021, allowing women access to abortion up until 12 weeks gestation, women are still struggling to gain proper access to legal abortion for free at public hospitals because doctors are unaware of the law or find excuses to delay the procedure.
Human rights defender and lawyer Ariadne Song has defended women’s rights cases for 19 years, including the ‘aborto legal’ campaign first started by the Green Wave, or Marea Verde, in Argentina.

How to Stop Taxing Our Families and Our Future
Children bring us happiness and shared hope for our future. Yet, the surest route to U.S. poverty is simply being a child or a mother. Other developed nations on average contribute $14,000 a year for toddler care. The U.S. invests $500. That’s not only stingy. It’s stupid.
Taxing women and their wombs hurts all of us. It’s a better plan to tax those who can best afford it.

We Must End Racism in Healthcare. Expanding Medicaid Is A Good Start.
Black women across America face many health crises buoyed by systemic failures ever-present since our country began. The fact that health disparities persist and widen is an indictment on our system and those whose health and well-being it prioritizes—but more is possible.
Closing the Medicaid gap is arguably one of the quickest ways to make our nation’s health system more equitable.

Let’s Save the Maternity Units Like We Do the Banks
What if we thought about maternity care like we thought about extractive, under-regulated, poorly run banks? We have plenty of examples of the federal government quickly mobilizing resources to bail them out. They are indispensable! They are core to the wellbeing of our economy and our communities! They are too big to fail!
But I can’t imagine many things more core to the well-being of our economy and our communities than the health of women, of mothers and the children they bring into this world.
Destroying Myths and Misogyny in Endometriosis Care: ‘Unless I Was Trying to Conceive, No One Cared About Bleeding and Pain’
In Tracey Lindeman’s new book BLEED: Destroying Myths and Misogyny in Endometriosis Care, Stephanie Lepage wonders how different her life could have been if only the doctors had bothered to look for endometriosis before her mid-30s. She had developed constant pain in her right lower abdomen that was so intense that rolling onto her side would shoot her out of a dead sleep on an almost nightly basis. When Lepage finally got in to see a gynecologist about it, that doctor said it was little more than a red herring. She remained in agony for two years without reprieve until it mysteriously subsided.
“The thing that stood out to me the most was like, unless I was trying to conceive, no one even cared about bleeding and pain.”