
Maternal mortality is a test of a society’s commitment to equality. The United States is failing.

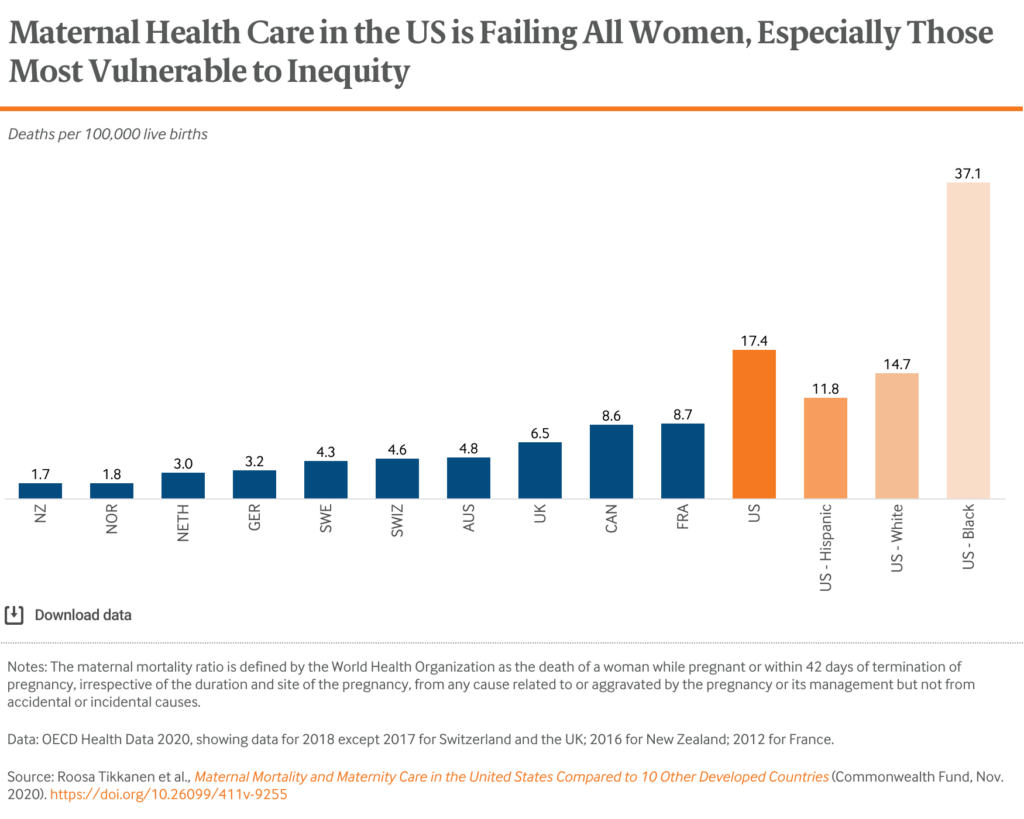
The U.S.—the world’s most expensive health care system—has an abysmal track record for maternal health and is an outlier among high-income nations.
- In New Zealand there are 1.7 deaths for every 100,000 births.
- In France, which has among the highest maternal death rates in Europe, there are 8.7.
- In the U.S., the number jumps to 17.4. And, if you are a Black person in the U.S. the rate is a dismal 37.1. The rates are similarly high for Indigenous people.
While the maternal deaths are perhaps the most shocking indicators of how our health care system is failing pregnant people, it would be remiss to not also look at rates of serious harm, injury or incidents where a person nearly dies during pregnancy and/or childbirth. These are similarly shocking and affect more than 50,000 women per year. And, while those who suffer these experiences survive, many experience lasting disability and are often forever changed by experiences of trauma.
Consistent Devaluing of Black and Indigenous Lives Results in Poorer Health Outcomes
Our health care system has suffered as much any other institution from this country’s history of systemic racism and gender oppression—with people who are at the intersection of both suffering the most. We can look at centuries of examples of mistreatment—from Tuskegee, to non-consented medical experimentation without anesthesia. The obstetrics profession itself has a horrifying history where advances were made through the torture of enslaved Black women and the displacement of community-based midwifery providers.
Generations of economic disinvestment in communities of color and under investing in health systems that serve people of color have had lasting negative impacts on maternal health care. In addition, numerous studies have described the unequal treatment of Black women when they arrive at health systems where calls for help are often ignored or devalued. It should be no surprise that this consistent devaluing of Black and Indigenous lives has resulted in poorer outcomes for them.
Current Policies Fall Short
Current U.S. health policies and practices contribute to high maternal mortality and injury rates by restricting pregnant people’s access to the health care. Currently, 12.5 percent of people in the U.S. are uninsured—and this number is rising as a result of the COVID-19 pandemic. Pregnant and birthing people here are not guaranteed to have health insurance throughout their lives, pregnancies and or into the post-partum period.
Medicaid, the federal health insurance program for people with low incomes, covers nearly half (42 percent) of all births in this country. In many states, Medicaid is difficult to qualify for—requiring recipients to have almost no income at all. While there are exceptions for pregnancy, they don’t last long. Medicaid coverage for birthing people runs out 60 days after birth in a lot of states—which is dangerous, as approximately half of maternal deaths occur in the post-partum period, up to one year after giving birth.
We do not have enough midwives and ob-gyns overall—and we have far fewer midwives than similar countries. As a result, parts of the U.S., both urban and rural, are maternity care deserts, where people cannot find maternity care close to home.
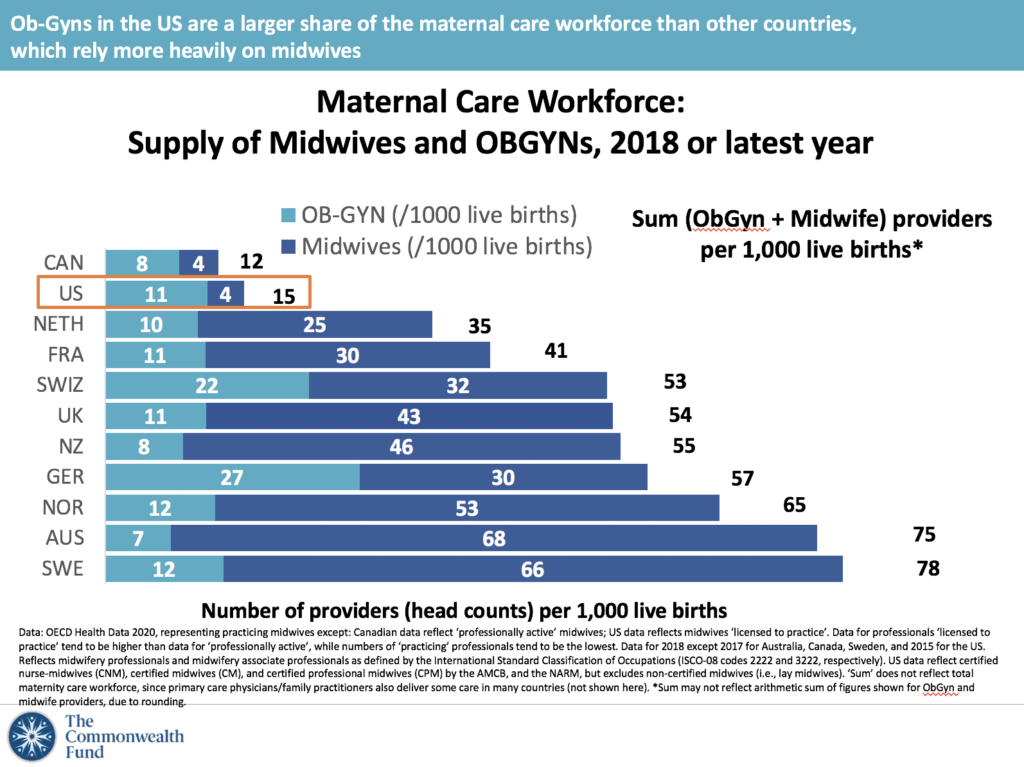
This short supply of midwives in the U.S. is compounded by insurance coverage complications, as coverage of midwives varies from state to state, making it an unaffordable option for many birthing people.
It is also worth noting the U.S. has very few maternity care providers color—only 6 percent of midwives are Black and only 4 percent are Latino; while only 11 percent of ob-gyns are Black and 7 percent Hispanic.
Lack of Paid Leave Is a Grave Danger for Many Mothers
Finally, despite the fact that research shows that birthing people that receive paid leave from work have better outcomes than those who do not, the U. S. remains the only industrialized country that doesn’t guarantee it. The minimum in other high-income countries is between 12 and 15 weeks in Mexico and Israel, while others, including Scandinavian nations, are more generous, providing more than a year.
The U.S. is also among the countries that provides the least financial support to families in terms of paid parental leave, child care subsidies and support to single mothers. In fact, we pay out about three times less than the average industrialized country.
Where Do We Go From Here?
With a new administration in the White House, we have a fresh opportunity to do better, and we should take it. A package of legislative proposals known as the Black Maternal Health Momnibus Act was re-introduced in Congress on Monday, but a path to becoming law is unclear and will require sustained leadership to keep this issue from being buried by competing priorities.
There are long list of “shoulds,” there are a few that truly stand out:
- We must address systemic causes of racial inequities so people of color and Indigenous people are not at risk when they are pregnant and giving birth. This begins with us dismantling structural racism within the health care system and our communities. A tall order but one that begins with us enacting policies that will improve living conditions, invest in communities, and address inequalities in health care access, quality and safety.
- Insurance coverage is a key part of any solution. Expanding the Medicaid program in every state would assure that millions more people have health insurance coverage throughout their lives. This will mean starting pregnancy healthier, and also having the access to preventive care and postpartum care that is so critical to a healthy pregnancy and birth.
- We need more maternity care providers, especially midwives. Rethinking laws and regulations that make it harder for midwives to practice autonomously and harder for insurance to pay for them is part of this. Investing in growing a diverse field of providers by supporting birthing centers led by people of color and providing pathways for people of color to enter the maternal health field is also essential.
- Universal paid family leave would be a game changer for pregnant and birthing people in the United States. Allowing new parents to care for their babies and themselves without worrying about lost income would lead to significantly better outcomes for families.
We have to do better for pregnant and birthing people in the United States. There’s no other option. Of course, we cannot erase the impacts of hundreds of years of race and gender-based oppression overnight. However, there are very real, concrete steps we can take to put the United States on the path to an anti-racist, equitable health care system where birthing people of all races and ethnicities have what they need for healthy, happy pregnancies and births.
You may also like:


